Neurological Assessment in NMC OSCE
Neurological Assessment in NMC OSCE
 Some candidates find it very difficult when they get neurological assessment for their assessment station in APIE Stations. Is there anything to be worried about? Do we need to do complete neurological examination prior to taking observations? Do you have to tell NEWS score of patient? Questions are many.
Some candidates find it very difficult when they get neurological assessment for their assessment station in APIE Stations. Is there anything to be worried about? Do we need to do complete neurological examination prior to taking observations? Do you have to tell NEWS score of patient? Questions are many.
This article will help you to know more about Neurological Examination to be done as a part of Neurological Assessment in NMC OSCE
Neurological Examination in Neurological Assessment Station
Scenario
Mr. X has been admitted in Medical Assessment Unit following a fall at home. Patient was found to be drowsy and confused at home by daughter. Ambulance crew brought patient to hospital. Now, patient is awaiting a CT scan. You are the nurse taking care of the patient and you need to do an assessment of patient including Observations along with neurological status assessment.
Introductory phase
As for any other assessment station, Do the hand rub using seven steps of hand hygiene and provide privacy to the patient.
Then you need to introduce yourself as the nurse caring for the patient, identify the patient using Full Name, Date of Birth and Hospital Number.
Ask for pain, if patient is complaining of pain, rate using pain scale (Note it down)
Also Ask for any allergies patient is having.
Ask about reason for admission to patient (don’t elaborate)
Before taking Observations
Ask few questions which will help you know the orientation of patient to time, place and person
Those questions are
Do you know where you are now?
Also Do you know what time it is?
Do you know what month and year it is?
After this, continue to take observations (BP, RR, PR and Temperature)
Chart all observations on the Neurological assessment sheet given by the examiner
After charting observations, tell patient that you need to do some more assessment to plan nursing care for the patient
Neurological Examination in NMC OSCE
Ask the patient to sit upright, looking straight
Ask patient whether he had any surgeries done in eyes?
Tell patient that you are going to flash a light on his eyes in order to view his pupillary reaction.(Torch will be supplied by examiner)
Flash light from outer canthus to inner canthus
Note the pupilary size and reaction on the observation chart
Ask the patient to clench his teeth
Ask the patient whether he had undergone any surgeries to back or shoulder
Tell the patient to straighten both arms
Press the arms one by one from top to bottom and vice versa against patient resistance
Note the power of arms on the observation chart
Ask the patient to straighten both legs
Tell the patient to lift one leg
Press the leg from top to bottom and vice versa against patient resistance
Do the same with other leg too.
Note the power of legs in the observation chart provided
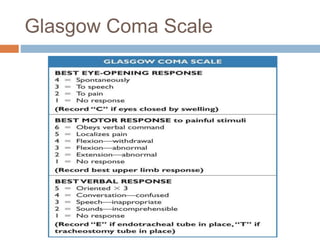
Complete the Neurolgical observation chart and calculate the GCS Score
Verbalise the GCS score to the patient and explain plan of care/escalation
You have to calculate NEWS2 score as well for the patient who you are assessing neurological status. For which, we can use ABCDE method of assessment.

‘ABCDE’ Method
While taking observations, you can go through the ABCDE method of assessment through the following steps
Airway: Clear; no visual obstructions.
Breathing: Respiratory rate; rhythm; depth; oxygen saturation level; respiratory noises (rattle wheeze, stridor, coughing); unequal air entry; visual signs of respiratory distress (use of accessory respiratory muscles, sweating, cyanosis, ‘see-saw’ breathing).
Circulation: Heart rate; rhythm; strength; blood pressure; capillary refill; pallor and perfusion.
Disability: conscious level using ACVPU (alert, confusion, voice, pain, unresponsive); presence of pain; urine output; blood glucose.
Exposure: Takes and records temperature; asks for the presence of bleeds, rashes, injuries and/or bruises; obtains a medical history.
Plan of Escalation
If GCS 15 – Every 30 Minutes for 1st 2 hours,
every hours for next 4 hours & every 2 hours
thereafter until stable and GCS maintains to 15/15
and escalate as per NEWS policyIf GCS 14 & Below – Every 30 Minutes until stable &
GCS reaches to 15/15 and escalate as per NEWS policy,Observe for signs of Deterioration
Do a final hand rub using seven steps of hand hygiene and leave the room.
Major pitfalls in Neurological Assessment
– Not getting enough time to complete assessment
– Forgetting to tell the GCS score to the patient
– Forgetting to sign off the Neurological Observation Chart
The Neurological Observation Chart for NMC OSCE

Conclusion
Neurological Assessment is a very simple station. You just need to do it in right way. Minimize over talking to patient. Watch for signs that actor will be giving off. For eg. some times patient will be repeatedly asking your name which give clue to confusion.
Don’t try to overdo neurological assessment by using all the neurolgical tests done by medical team. You can simply pass the exam by only following the neurolgical examination steps detailed above.
We are also giving a link to the video that we have made to make your remember neurological examination easily – See the video
Please note that time for assessment station has changed from 15 minutes to 20 minutes now